I'm very overdue for an update, a blog post, an anything...so buckle up!
The Good
Some of you may have seen the exciting, official unveiling of the Global
Mercy (GLM)! This new, state-of-the-art, built to purpose vessel will more than
double the organization's capacity to provide free surgery, and includes some
really fantastic features to improve our training capabilities (like a snazzy
simulation lab)!
But don't just listen to me talk about it...take a look!
I'm pretty darn excited about it! The hospital layout is going to be so much better - not just for us, but for our patients, as well. They'll have WINDOWS, a veranda they can always access, and overflow beds for caregivers. The wards have an enclosed nursing station, which is much nicer for night-shift, and will have computer stations for charting! That's right - we're moving into this century with digital charting!
The GLM just completed its first 'Sea Trials' where the engines & maneuverability were put to test, and exceeded all expectations. I'm looking forward to getting to know this ship when the transition happens - tentatively planned for late next year!
The Even More Good
Even better news, the BBC recently reported on the success of the government, professionals, and people of Senegal at keeping COVID-19 at bay. Several key factors here: they have an incredible infectious disease center (L'Institut Pasteur) which has developed several testing options (including an inexpensive, 15 minute test). They also were able to more than double their ICU capacity. Hearing that they started with only 10 - 12 beds equipped to care for COVID patients definitely drove home how vital it was that our crew not end up taking any of those much-needed spaces. Leaving was tough, but it ensured we would not become an avoidable burden.
The Bad
Unfortunately, COVID is still making it challenging to pick up where we left off. International travel is hard, and - for most people - may involve quarantines on either side of said travel. In the pre-pandemic days, we relied tremendously on short-term volunteers who spent as long as a few months to as little as two weeks on board. It's pretty hard to ask someone to leave their normal workplace for 6-8 weeks for only 2 weeks of actual service.
These factors drove the decision to postpone our return to April 2021; although as that date creeps closer, I'm still wary of how unpredictable this pandemic has been. Vaccine rollout is promising, but is still months away from having much of an impact on transmission.
The Unknown
So, here we are. The strangest Christmas in my lifetime after the most challenging year of my lifetime. I am incredibly grateful for everyone who helped support me through this unexpected furlough - from the trailer I was able to quarantine in, to family letting me bring my laundry over, to temporary job opportunities lining up and a living space falling into place. I have joined a reservist roster with the Red Cross, and so expect to be doing...well, something, with them come the new year. Could be COVID testing, could be vaccines, could be something else entirely! And where in Canada that will be is just as much up in the air. As is so often the case, though, the opportunity seemed to fall in my lap right when I was debating what to do next. So I am most grateful for someone who knows my needs before I do, and who always has a route mapped out, though I can only see the next few steps.
*cue relevant Disney musical number*
I am still tentatively signed up to attend On Boarding, the Mercy Ships training program for long-term crew, come March. This takes place in Texas, and I'm sure you can imagine my hesitance to travel anywhere in the US at the moment! I'm trying my best, though, to trust that map that I can't see, and the One who has already charted the course.
Thank you to all who have and continue to support me in this journey. I will leave you with this very awkward bundle of great memories from this time last year, and wish you all a very Merry Christmas & Joyeux Noël.
It's been almost 2 months since the AFM departed Senegal for Tenerife, and I thought I should fill you in on what's been happening since.
First news first: I have a tentative return date! I hope to be flying home on June 4th. I have found a place to safely quarantine before I re-enter this strange new version of home. I am seeking some sort of (ideally casual) work to keep me busy while we wait to find out when we can return to Africa.
There have been flurries of activity and quiet lulls on board, exciting days and tough days, but I'm grateful for friends that are still around while many have made it home. I'm also grateful for many activities and new places to work which have kept us busy and entertained during these interesting weeks.
My new work team! The AFM receptionists with our amazing Purser & Assistant Purser (ctr, ctr right)
Captain photobombs are best photobombs!
...we have fun keeping the ship safe.
Our hard-working galley crew now includes nurses, physiotherapists, & a dental assistant!
Our amazing Nepalese crew cooked a special dinner one night for the whole crew!
We played this pictionary-style game (with a secret twist) at one of our farewell dinners. Any guesses what either of these pictures are?
Our little walking track (must stay within the pylons & keep 2m from each other)
Shredding! Copious amounts of shredding of old, sensitive documents! Went through at least 3 of these jumbo bags.
Part of a thank you to our port agents for all they have done helping us settle in here! Each section of each letter was coloured by a different crew member.
So many beautiful sunsets over the mountains!
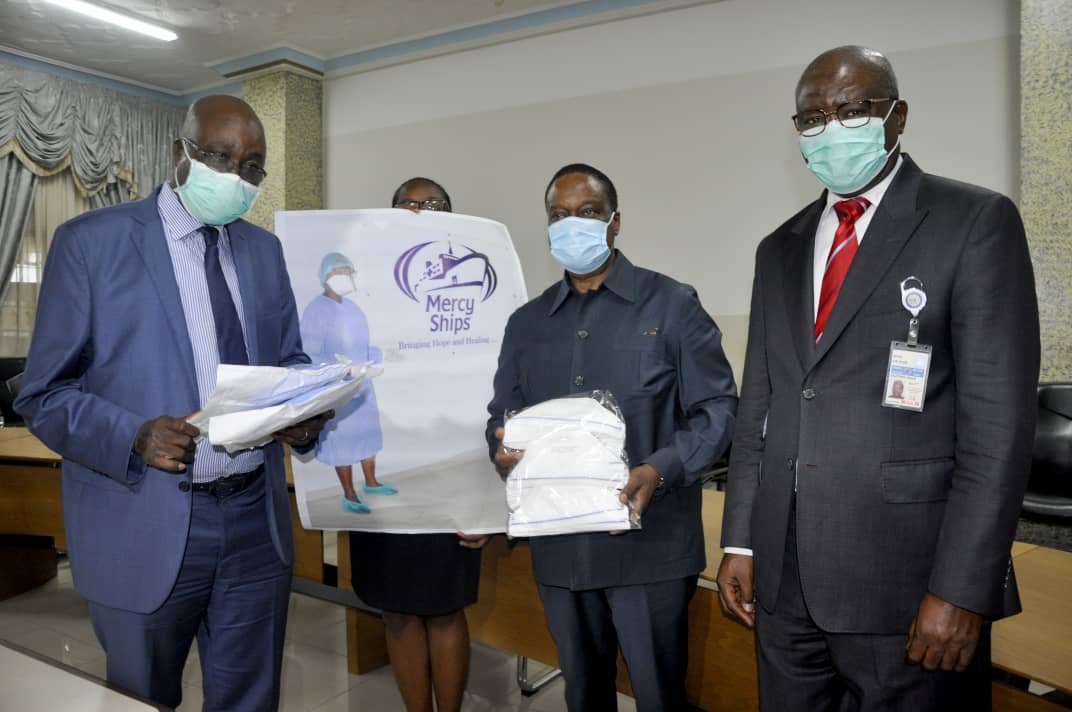
Although our primary work has had to come to a stop, we've tried to find ways to continue helping the nations of Africa, and the one that we're in! Our Africa Bureau has organized donations of PPE and essential medical supplies (that were intended for use in Senegal these last 2 months) for the Health Authorities of Sierra Leone, Madagascar, Liberia, and Benin. We also continue to follow-up & check-in on the progress of our patients back in Senegal, via our day crew and other local contacts.
Donated supplies in Benin including surgical gowns, masks, gloves, caps, and eye protection.
This photo keeps popping up on MS social media but I feel so bad for the lady holding the poster!
More supplies ready to ship to Sierra Leone
MS alumni, Dr. Odri Augbessi is spearheading a public awareness campaign in her country of Benin.
Dr. Sarah Kwok hands a donation of PPE over to the Spanish Red Cross
Hopefully that helps give you an idea of what's still going on over here! We're doing our best to stay busy, and help where we can.
And, in case you missed it, here's the overview of what we did accomplish before leaving Senegal (See if you can spot me - I made it in there twice)!
Looking forward to being 'home,' although it will certainly be an interesting adjustment.
As I was going about my business this morning (enjoying a rare opportunity to stream some of my favourite tunes while the internet holds up) I reached for my multivitamins and was reminded of something. A small detail from over a month ago that was lost in the fog of chaos at the time. I opened the safety cap, pressing down and twisting, and was brought back to the beautiful, weathered & wrinkled face of an older woman.
I don't remember the details of the patient - heck I'm not even sure which specialty they were - other than it was a child with an elderly grandmother as a caregiver. They had several liquid medications; as I was working through each one, explaining their purpose, when to give them, and how much, we came across a bit of a snag. Grandma was a champ with all the details, repeating the information back to me perfectly. But then I asked her to practice giving a dose of paracetamol.
It's not uncommon for people to have trouble with the child safety caps the first time they encounter them, which is exactly why I asked her to give it a try. This dear woman, though, despite multiple demonstrations & explanations, just could not get that cap to open. My translator and I spent a good 5 minutes on it, and though she continued to smile and laugh through the struggle, I could tell she was getting frustrated. She even tried to fake us out a few times, spinning the cap and nodding as if she had gotten it!
Finally, I reached across my translator to take the woman's hands into mine. I held the bottle, pressing her hand down on the top, and we both twisted together, successfully getting the lid all the way off. We did this once more before she was able to finally get it done on her own, multiple times, and I was confident she would be able to manage at home.
Such a trivial part of my usual day was a nearly insurmountable task for that woman. It was something she couldn't work out without experiencing what the mechanism felt like. Something no amount of explaining or demonstrating could achieve. We needed to walk together through the process, doing the work side-by-side - or hand-in-hand, in this case.
This woman was teaching me, although it took it a month to sink in, an incredibly important lesson.
Loving, serving, teaching, 'helping...' can often be a self-serving exercise that feels good for us but leaves no lasting impact on others. It's not enough to throw money at a problem, to say some half-baked platitudes, to say, "I'll pray for you," if we aren't willing to walk through the challenge with them. Empathy is one of those concepts they talk about a LOT in nursing school. I don't think it's importance can be overstated in this profession, but I also don't think it's something that can be taught in a classroom. It's something you have to experience. You have to stand awkwardly under the wing of a more experienced nurse while they help a patient through pain - physical, emotional, spiritual, or social - and you begin to understand empathy in practice. You have to resist the urge to laugh at what might seem a stupid question, and realize how unsettling and scary it would be if you didn't know the answer. Your patients teach you how to imagine their experience through their eyes, and walk together with you down this road of better understanding.
I started this post before the Covidsanity began - with the intention of making an announcement.
Fearless TL Brittany with Babacar - one of our favourite patients from this year!
My amazing supervisor, who has been expertly leading the general ward nurse team for the last 3 years now, is taking a break from her service here. A gap opened up, and, somehow - after a lot of prayer & a fair bit of uncertainty - I got poked/prodded/coaxed into applying for it. Coaxing & prodding seemed to be coming from a few sources, but there were a number of coincidences (which I really don't think were coincidences) that gave me such a strong sense of direction in this matter - I couldn't ignore them.
As a result, I can finally announce that I'm going to be returning to work with Mercy Ships for their next field service as the Ward Nurse General Surgery Team Leader! Although she is (slightly) shorter than me, Brittany leaves VERY big shoes to fill, and I'm exited yet nervous yet eagerly anticipating joining the phenomenal ladies that make the hospital wards run.
Now, you probably have questions: Q: Whaddaya mean 'returning'...aren't you already there?
A: Yes, yes I am. On the ship, that is. In Spain. Docked at a jetty. That I can only set foot on to throw out my trash. As our field service ended early, I'm working on plans to return home sometime around the end of May or beginning of June. I was supposed to be heading to Texas for some training before returning to the ship in August. Thanks to the current state of the world, exact time frames are a bit...vague...at the moment but as soon as it's possible to start serving the people of Africa again, that's where I'll be. In the interim, I'll be looking for temporary work in Canada.
Q: Returning...where?
A: Our hope is to return to Senegal to complete our planned surgeries. We left on very good terms and have a strong relationship with both the Ministry of Health and the president, and will do everything we can to fulfill our commitment to them, once it is safe to do so. After that, the next field service is planned for Liberia - a country I'm really looking forward to serving and learning more about. Bonus: English is their official language!
Q: What exactly will your role be?
A: Each surgical specialty we do on board has an OR Nurse Team Lead, and a Ward Nurse Team Lead. They work together to coordinate patient care on both sides of surgery. Most of our surgeons, nurses, and anesthesiologists come and go throughout the year, staying only for a couple months or even weeks. Team leads help maintain consistency through all that changeover, supporting the nurses & surgeons as they jump in for their time on board. They act as a line of communication between the ward nurses, OR nurses, surgeons, anesthesiologists, chaplaincy, and the hospital leadership. They also can see more of the big picture of each patient's journey, anticipating their needs and planning accordingly. It also means I get
Q: 'General' Team Leader - does this mean you outrank the Captain?
A: The Master (Captain) of a ship always outranks everyone. ;) The General Surgery* ward, though, has been my home for this past 8 months, and is a good place to get a little bit of everything. General Surgery (in this context) = hernias, lipomas (soft tissue tumors), thyroids/goiters, and the occasional mastectomy. As most of those are quick turnovers, we also get overflow from nearly every other specialty. Oh yeah...and we get those adorable pediatric cataract patients, too.
*One of my old roommates got me into the habit of saluting whenever a military rank casually drops into conversation, just 'cause. Like if you found a popcorn kernel. Or had a private conversation. Or you were having major difficulties with keeping your blog post on topic. This is a trend I fully intend to indoctrinate all my nurses into - whenever General Surgery is mentioned. I hope they don't all hate me. Q: How long?
A: This is a very hard question to answer in the midst of these uncertain times, but I plan for another year at the least, two if possible. It's hard to know what will come that far down the pipeline, and somewhere in that time frame there's going to be a changeover to a new ship which might shorten or extend my plans. For now I'm just going to trust that at the right time the right path will be made clear.
Clear as mud? That's about how I'm feeling too. Probably how the whole world is feeling right now.
I'm so grateful for all of you who take the time to read this and check in with me, and keep running alongside with me as I make rather unconventional life choices. Y'all (oh dear, the American crew are rubbing off on me) have got my back, and I can feel you there, propping me up when I falter, on a daily basis.
Thanks for being there. Thanks for reading this. Stay safe out there.
I started my day charging (manning the desk, essentially), in A Ward. Half of the ward is filled with plastic surgery patients, all splinted and bandaged up, waiting for their skin grafts to take root and mobility to improve. The other half of the ward is max-fax (facial surgeries) with a lot of drool and swelling and feeding tubes.
4 of our patients are well enough to be discharged from the hospital.
One problem.
PANDEMIC!
At an all-crew meeting yesterday (Friday the 13th, no less...), a panel of our hospital & operational leadership delivered the news that surgery was being stopped, our programs would quickly wind down, and we'd prepare the ship to sail as soon as reasonably possible. The room was dead silent. My friend Maddy, a screening nurse (I've talked about before), was sitting next to me, grabbed my hand and started squeezing. I know, in her mind, she was racing through the hundreds of patients who had been scheduled to come for surgery in the next few months. Over the next week, they would all be called and told the unfortunate news. The 60+ who had already arrived to the HOPE Center who would have to be sent home.
Heartbreak is an understatement.
It was difficult news, but I think it was the only sensible option. So many of our crew are itinerant; our programs depend on dozens of new arrivals, from around the globe, every weekend. In the current outlook, that was going to become increasingly risky - if not impossible. Not to mention how devastating it could be if such an infectious contagion got on board. This was the right choice.
But that didn't make anything about it easy.
---
During my shift, the 'bing-bong' of the ship-wide PA went off heralding this announcement: "All shore leave is cancelled. All shore leave is cancelled. If you know of any crew ashore, please contact them to return immediately." We later learned that from our 250 day crew who usually help in all our departments to keep the ship running, 53 were asked (if they were willing) to stay here with us as temporary crew. They would live in a tent on the dock or in our admissions ward - on mattresses on the floor. They would stay in our quarantine 'bubble' to help with the final essential tasks (not the least of which was caring for and providing information to our patients before they left).
At the end of the day, though I probably should have been sleeping, the day's news and events kept me thinking there was things I should do. I scrounged some extra toiletries (including those of a cabin mate who was unable to return from her 2 weeks of time off), and headed back in to the hospital. All 20 steps. One of our team leads had suggested we bring some donations for the day crew who were unable to get home before hunkering down with us. They had toothbrushes, toothpaste and soap from hospital supply, but that was basically it. They worked a 12 hour shift then agreed to just stay on for the next 2 weeks without seeing their family. Or getting a change of clothes. Not a single one complained.
They are my heroes.
Walking down the hall, I passed a patient I had cared for the past couple of days on D Ward. She had been missing the whole part of the lip that sits under the nose - a rather more extreme type of cleft lip. Dr. Gary cut and stretched and built her a new one. She was still a bit swollen, but when she saw me, her face lit up. We exchanged greetings, I told her she was looking beautiful, and she gave me the most unexpected but wonderful, french-style, hug-on-this-side-then-hug-on-the-other hug I've ever had. Plus a little dance to boot.
In the midst of the days chaos; all the uncertainty and worry, that moment stood out as quite possibly the most important thing that happened in my life that day.
3 Days Later...
I'm sitting on the floor, leaning against a bag of blankets, pillows, toiletries and gowns, ready for a patient that will be transferred to a local hospital the next day. Several other nurses, and our rockstar nurse team leaders are sitting nearby, all of us spent. We've transformed the now-vacant Opthalmic Team room into our Master Control Center for the biggest exodus of patients I've ever been involved in. 53 patients were on board when the decision was made to shut things down. At least 30 of those still required complex wound care, physiotherapy, and medical follow-up. 3 of them needed another surgery before they could leave. ALL of them needed documentation, dressing supplies, medication, nutritional supplements, transportation, and thorough teaching about their self-care. One of our biggest challenges is: 'how are they going to CARRY all these cans of Pediasure!?'
The first few days were stressful beyond belief, with our team leads working 16 hour days to get things in motion. We are so grateful to have strong partnerships with a number of hospitals & clinics throughout Senegal, who were willing and able to accept our patients. Transferring one or two patients, who just need a little more time, at the end of a field service isn't unusual. Transferring this many, though, was unprecedented.
Our 'Discharge HQ' - plans for each patient plastered on the wall. The bags are for hospital transfers are under the table.
Bags upon bags of dressing supplies & nutrition supplements. Most patients took at least 2 of these bags home.
Team Leader Brittany ticking off the 'Left the Ship' box - cause for a small celebration at the end of each day.
1 Week Later...
Our last 5 patients have made it out the door. All the remaining nurses on the ward, mostly working all day to clean & pack up, paused to clap them off. We started out in a mad frenzy, but every day got a little bit easier as our planning and preparation smoothed out (almost) every wrinkle. Still, we are exhausted. Physically, emotionally, and mentally. In the midst of our focused drive to do the best by our patients, over 200 crew members left to get home while they still could. Every day, it seemed, another group of cars would head off to the airport. So many goodbyes were said not knowing when we would see each other again; sometimes knowing we'd likely never see that person again. The future beyond the next 12 hours was as unknowable a thing as the number of hairs on my head. Every time the PA 'bing-bong' went off, we all flinched, wondering what new wrench in the works it would be this time.
The biggest encouragement - the thing that kept me going through each of these non-stop days - was the patients. Every single one of them, when we'd finished cramming their heads with information about diet and mobility and wound care and preventing infection and what to do if they had problems...every single one said 'jerejef' (thank you). But not just 'jerejef' - it was a deluge of thanks and prayers and blessings. 'Jerejef. You've done such good things for us. We are so grateful for how you've looked after us. Jerejef. Jerejef. We pray for your health, for your family, for the whole crew of the ship. Don't be worried about us. Jerejef. Peace be with you. Peace only.'
- Lin Manuel-Miranda
---
An article from Al Jazeera popped up on my newsfeed: "Senegal shuts borders amid WHO fears Africa is next virus hotspot." I took note to watch the video later. When I do, I'm surprised to see the Africa Mercy come on screen. "Even the United States' Mercy Ship, a floating hospital with 400 nurses and doctors on board meant to offer help, is leaving Senegal when it's needed the most."
SERIOUSLY. I can't believe my ears. So much misinformation crammed into one sentence. We're not affiliated with the US, we're an international NGO. There are probably fewer than 100 medical personnel that make up the 400+ crew. The help we offer is elective surgery to correct chronic, debilitating conditions. We are NOT equipped or qualified in any way to intervene in this situation. Not to mention that, as has become painfully evident from the cruise ship debacles, ships are NO PLACE to try to contain this virus. We are leaving with the full approval of Senegalese Minister of Health.
We hated that we had to leave. We desperately hope, as we say our goodbyes to daycrew and patients, that this is not the last time we will see them. But it's out of our control. We have to say goodbye. Staying could do more harm than good.
I send a very pointed comment to the editor. I hear nothing back.
2 Weeks Later...
We are about to sail.
We're now only 239 souls (including enough children to keep the academy running). It seems like a big number, but it feels eerily empty and quiet. Instead of a packed out dining room at lunch, there's only a smattering of people around. Nurses that didn't make it home have all been reallocated to other departments - it's very strange seeing them out of scrubs and instead in a galley or housekeeping uniform. I end up (after a couple days 'rest' where I don't know what to do with myself) transferring to reception. This is usually a very busy position overseeing arrivals and departures, but at the moment it's almost entirely answering the phone and keeping an eye on the fire safety system.
New job, who dis?
The hospital is packed and strapped in for a rocky sail - but much of the usual cleaning was cut short and will have to be completed sometime down the road. The normally restricted OR corridor is wide open, changing my usual route to the hospital offices. It's very odd walking through there in normal clothes. I do a little admin work for the hospital to fill the downtime. It's hard to not be working after such an intense period of life.
24/7 stowaway watch to ensure no uninvited passengers come aboard (standard before any sail). Good time to think.
The sail is lovely. The ship is extra empty; everyone with bad seasickness just stays in their cabin. It only takes us 4 days to get to Tenerife, where the Spanish authorities have permitted us to dock (but remain quarantined on the ship). Reception has shortened hours while sailing, so I have a lot of down time (and, fortunately, don't get seasick). Time to think. Time to sleep. Time to watch for whales breaching or dolphins skipping alongside the bow. Time to soak in the spectacular sunsets.
Today.
Life on board is getting back to the 'new normal' - new routines are starting to slowly settle into place. News still rolls in, but it does so in gentler, lapping waves instead of crashing breakers. Plans & possibilities for the future are beginning to formulate and emerge from the fog, though a great deal of mystery is still clouding the view. For the time being, I am hanging tight here on the ship in Spain, until such time as I can get a break at home, or we can return to our work for the people of Senegal.
I am incredibly grateful for the people around me, for their grace, their incredible drive, and for holding me and this ship together.
I am grateful for chaplains and friends, checking in on each other and carrying each other through the hard days. I am grateful for the planners, who are keeping us busy during our 'isolation vacation.' I am grateful for family and (albeit spotty) internet that can keep us connected across the globe.
I am grateful for the first rule of flying...and that it can be applied to a vessel of the sea as well.
Back in Cameroon, I did a couple of posts about some of the MVP's - most valuable patients & people. I thought I could continue that theme, as there have been SO MANY memorable people who have touched my heart, and whose stories should be shared.
Let's dive in, shall we?
The Best Mover & Shaker
When I first met Modou, he was curled up in his bed, blanket pulled over his head, his breakfast untouched on his end table. His sleep cycle was completely out of whack, he was struggling with motivation to eat, get out of bed; more than a little bit of a slump - he had classic symptoms of depression. He had had a long journey, and still had a long way to go.
An accident as a young child left Modou with severe burns to his face, neck, arms, and hands. It is a fair miracle he survived at all; burns to the face often go hand-in-hand with burns to the lungs & airways. These can very easily be fatal without intensive treatment. Modou, clearly, did not receive much (if any) treatment for his burns. Scars and muscle contractures essentially tied his chin to his right collarbone, and his fingers were mostly gone. Only a few little nubs were left on the stump of his left arm to indicate where a finger and thumb might have been. Looking through his chart, there was a furrowed brow and a hardness in his eyes in his pre-op medical photos. It is a stare which many patients have in these "before" photos. It is, far deeper than physically, not a person I recognize any more.
Modou's first surgery tackled the contractures of his face and right hand. Numerous skin grafts were needed to build new, healthy skin which would replace the scars. As such, he had wounds on almost every limb - some where donor skin was taken, others where it was placed.
Modou (L) after his first surgery
After his first surgery, Modou's first few weeks were a struggle. There was very little he could do for himself, as both hands were bandaged, and he still had very limited mobility in his fingers. It was incredible, though, how well he could balance a cup on his stump without spilling. We leave the dressings wrapped, untouched, for 2-3 weeks after plastic surgery; helps prevent infection, giving the grafts time to heal without any outside interference. This meant for over 2 weeks, Modou was just sitting in the ward, waiting. No windows, minimal contact with the outside world, only an hour of fresh air every day. Nurses and dietitians constantly hounding him to eat more, take his supplements, check his circulation, etc. It's no wonder the guy's circadian rhythm went haywire.
It took some sleep aids, some chaplain counselling, and eventually his mom staying overnight a few times to help get him into a better headspace. And just in time, too. Plastic surgeon Dr. Tertius had decided to offer Modou another surgery on his left hand, to give him as much function back as possible. They would also do a little more work to improve his face. This meant ANOTHER 2-3 weeks (minimum) on the ward. Nonetheless, Modou agreed.
In these photos, you can see that modou now has a thumb sticking up out of his left hand! If you feel the meaty part of your hand - between the thumb and index finger - that is where Dr. Tertius cut down into to separate the 1st metacarpal bone (all that remained of his thumb) from the rest of his hand.
While Modou would still have good days and tough ones, overall he grew more and more cheerful, optimistic, and stubbornly pushing through the harder tasks & rehab exercises.
More than anything, though, Modou LOVES DANCING. Nothing could get him, and everyone around him, in a good mood like a good beat. Nobody could match his moves. And he'd always don his traditional, black & white hound's tooth robe whenever dancing was happening.
Demonstrating some traditional West African dance moves
Joining in the Bambalela during a birthday party
Jamming to the djembe with a hospital chaplain on Deck 7
3 Months Later...
I had the privilege of being the nurse to decide, on a rare shift in the Outpatients tent, that Modou's wounds were completely healed, and he could be discharged from our care. He would still return for physical therapy for several weeks, so it might not have felt momentous to him, but it sure did to me. I was able to look him in his knowing eyes, say "everything looks perfect," and give him one last high-five/handshake/hug.
I have a lot of memories of Modou, from the Senegalese name he gave me (Mariam Seck), to the other nickname he gave me ('LOTION!' - owing to my constant nagging that he needed to put lotion on his graft donor site), to the chirps and bird sounds over my shoulder while I worked on the computer. More than anything, though, I will remember his eyes. The eyes that stared from his admission photos - distant and cold, his brow furrowed; becoming the eyes of a friend - trusting, mischievous, kind, and permanently smiling.
Modou came to us as a young man covered in scars; scars which held him back, forced him to depend on others for all his needs, and caused him pain to the point where only his mother's presence would comfort him. He left us with different scars; scars which granted him joy, freedom, independence, and confidence. Modou will never look "perfect."
A wonderful summer at home with gardening, beach dates, work, yard sales, and brunch
Crossing an international border and great lake by tiny car ferry
Catching up with friends from abroad (and explaining to the TSA agents that I was meeting friends from Africa...but they're actually from New Zealand, but they live in the UK...)
Returning to the ship in Senegal
Rehearsing and performing acapella with the Key of Sea
Transforming empty, packed-up wards into bustling centers of care & healing
Being given a Senegalese name by a plastics patient ("Mariam Seck")
Sharing a traditional Senegalese meal of Thieboudienne at our day crew's home
Getting to document our patients' journeys as a ward photographer
One of my fav photos
Living around baobab trees - enjoying their fruit, their beauty, their canopies!
Cucumber Nativity (ask me later)
Watching Modou (a particular plastics patient) dance
1 second a day from my time in Senegal!
-
Now, I did promise a bit of Q&A about screening back in December, and I was able to quickly chat with Screening Nurse Maddy.
The Q&A's of Yes's & No's
Q: How does screening work here in Senegal?
A: The Senegal Ministry of Health decided to run their own pre-screening, selecting about 1000 potential candidates in each of the 13 regions. This resulted in over 13,000 patients for us to see, which we did over the course of about a week in each region. About half of the screening team goes upcountry for these screenings, while the rest of us work here on the dock. Only about 1 in 10 patients we screen will get into the dockside screening. The vast majority are no's - but in many cases it's a simple matter of 'we don't have the right kind of doctor to fix the problem you have.' Those are easier no's. The hard ones are when we could help, but we've simply run out of space.
Once they get an appointment for dockside screening, we'll give transport money to help them get to Dakar (if needed), and a lot of them will stay at the HOPE Center. They're seen one more time on the dock to do a more thorough nursing assessment, and sometimes to start treating any co-morbidities (like high blood pressure) that might make surgery more risky. Sometimes we have to delay their surgery to follow up on something, like a patient recently who had a large wound on their leg. Goiter patients need several months of medication before surgery, and monitor them every week.
Eventually, when the surgeon for that specialty arrives, they'll see every potential patient on their list, and decide exactly what surgery will be done (if possible), and when. Then they're passed on from us to the Admissions team.
Q: Have you ever gone out of your way to make space for a particular patient?
A: Yes. Sometimes we know we only have 10 slots for a certain specialty on a certain screening day, and I'll try to hold out for the patients who could benefit the most. I remember seeing Mohammed in line and thinking, "That's a good one for Dr. Gary, we've got to save a space for him!"
Mohammed before (above) and after (below) surgery to remove a facial tumor.
Q: Do you ever refer patients you can't help to a local hospital?
A: Yes, but it depends. Although we try to make our information campaigns clear that we treat mostly chronic injuries & conditions, we still have patients arrive at screening with what is clearly an acute illness. Something that should be treated within days. Local hospitals are better equipped to treat these types of problems than we are on the ship, and in a more timely fashion (our surgery dates are often months after the screening has taken place). If we find a minor problem, we may recommend the person seek help from a doctor when they can. If it is a major, potentially life-threatening problem, we can and have arranged transport to a hospital and transfer care to a local physician.
A little peek into screening in Senegal with Christelle, a Ghanaian screening nurse.
If you're interested in the nitty-gritty stats of screening, plus numbers from all our programs so far in Senegal, check this out (click to embiggen - or try this link).
That's all for now. Sorry for such a long radio silence! À la prochaine.